(written July 2, 2009)

The monsoon rains have been delayed this season and reservoir levels are dropping, affecting accessibility of drinking water in the region, crop production, and the hydropower on which this area depends. We have been mostly without electricity here in Kenchanahalli.
According to the Deccan Herald, Wednesday July 1, 2009, power cuts will continue across the Karnataka state as we await the late arrival of the monsoon rains. The delayed rains are having an impact on power shortages throughout the country, and many states have banned private producers from selling power out of state. The Deccan Herald further reports that with the current reservoir levels (see chart below), power can only be generated for another week; if the low water levels cause generation from the hydroelectric power stations to cease, Karnataka state will need to purchase at least 30 million units of power (units not specified) daily and will be facing further power outages.
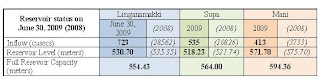
Note: adapted from the Deccan Herald, July 1, 2009, p5

In addition to the reservoirs that serve Karnataka listed in the chart above, the Kabini Reservoir and Dam were constructed in the 1960s, providing hydropower to the growing areas around Mysore. The Swami Vivekananda Youth Movement (SVYM) clinics in Saragur and Kenchanahalli where we are working serve tribal communities, many of whom were displaced through the development of the Kabini Dam and the designation of the surrounding area as a tiger protection reserve that forbids human habitation. For 30-40 years, these tribal communities have been living on the margins of modern society, attempting to maintain cultural traditions in displacement.
Tribal communities is the term used by local NGOs, the government, and community workers to refer to the populations that were traditionally forest dwelling. These displaced populations are particularly vulnerable to exploitation and poor health in the forced transition from traditional ways of life to surviving in a modernizing society (source: SVYM brochure and video).
[see later blog entry for an update about the arrival of monsoon rains]



